

Prior to my two Covid articles in mid-January (available here and here), I contacted the Ministry of Health for comment. I have now received their response and have set it out below along with some of my own additional observations. Some queries have been redirected by the ministry to the Office of the Minister of Health for additional comment and will be provided to me in due course.
1. What prompted CV TAG to change its recommendations made on 3 August to vaccinate high risk sub-groups in the 12 to 15 year old age range, to then deciding on 12 August (by email) to vaccinate all 12 to 15 year olds?
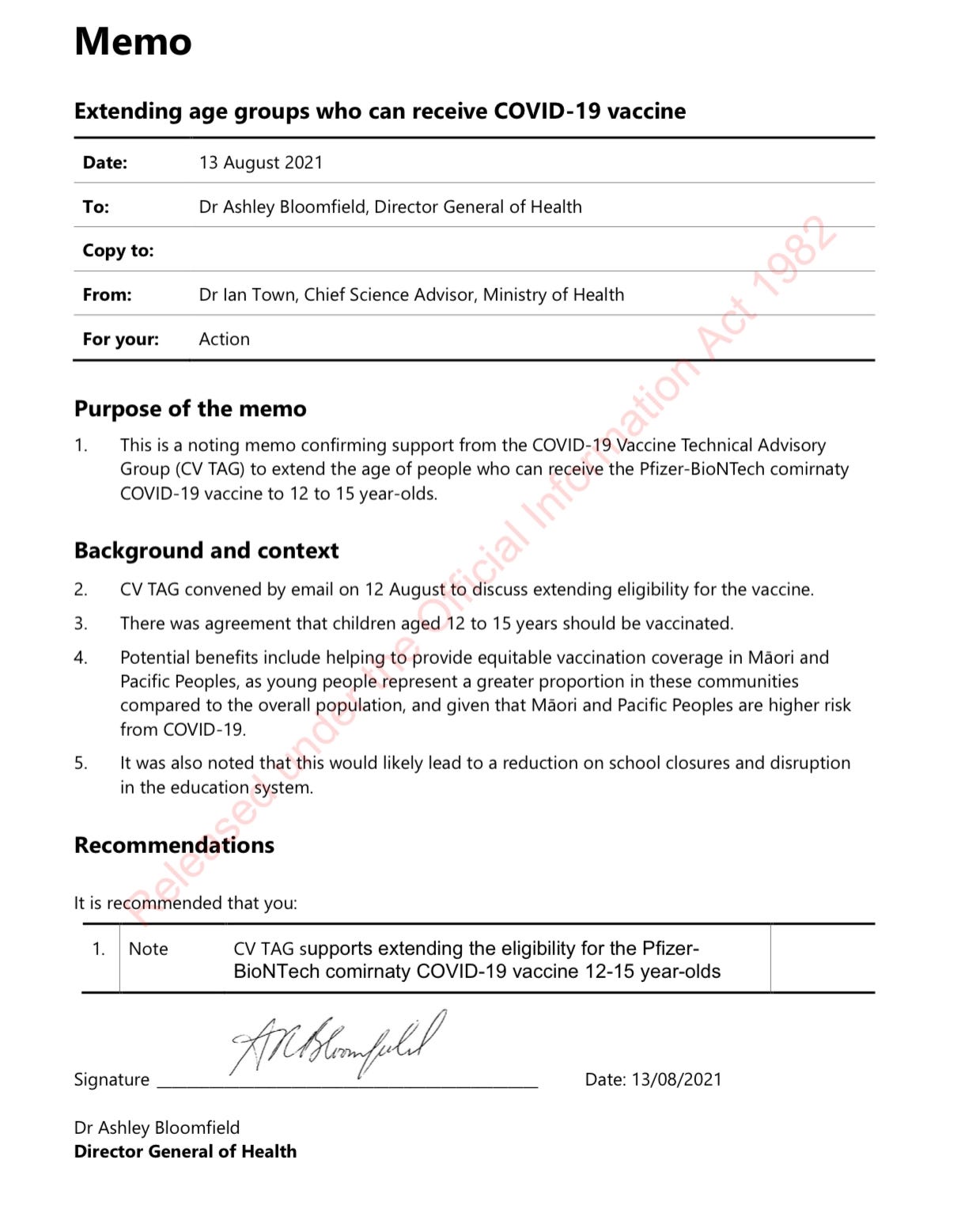
“Evidence of Covid-19 is rapidly evolving, and recommendations are updated as new information becomes available. The discussion by the Covid-19 Vaccine Technical Advisory Group (CV TAG) on 3 August 2021, was limited to vaccinating priority groups among 12-15 years olds. As stated in the CV TAG memo ‘Priority groups for vaccination among 12 to 15 year olds’, CV TAG will make recommendations for use in all children in the 12 to 15 years age group at a later date.
After this session, CV TAG reviewed additional evidence in relation to the broader age group, including advice from peak bodies internationally, and a review of safety and reactogenicity of Covid-19 vaccine among adolescents. As this was an issue needing urgent consideration at the time due to the threat of a Delta outbreak, CV TAG discussed and reached a resolution outside of meetings to offer vaccination to 12 to 15 year olds.”
It remains unclear what prompted the sense of urgency to emerge between 4 August when the CV TAG memo was issued recommending vaccination of high risk groups in the 12 to 15 year old age group, and 12 August when an extraordinary decision was made by email outside of the advisory group’s scheduled meetings to vaccinate all 12 to 15 year olds.
Unlike all other CV TAG memos which set out the information reviewed by the advisory group for each recommendation, the memo issued by CV TAG on 13 August neither sets out, nor refers to, the review of any advice from any international peak bodies or the review of any safety data. Nor does it note what prompted the urgent nature of the advice, particularly given that this occurred before the community outbreak of Delta.
Click image to view
2. Why did the government not implement the recommendations set out in CV TAG’s memo of 21 July 2021 to increase the dosing interval between the first and second doses from three weeks to eight weeks in order to reduce the risk of myocarditis?
“While Manatū Hauora (the Ministry of Health) does create advice informing Covid-19 policy based upon the analysis of expert bodies such as CV TAG, the final decision about the implementation of that advice lies with the Minister of Health, Minister of Covid-19 Response and Cabinet.
It is important to note that the decisions made in New Zealand’s response to the Covid-19 pandemic are influenced by a myriad of factors beyond advice from CV TAG. These decisions sit within the wider framework of epidemiological, economic, legal and political considerations. In addition, the wider context of the state of the pandemic is important to keep in mind. Of note, CV TAG’s recommendation was made in the context of the New Zealand setting in July 2021. The situation in New Zealand changed in August 2021 with the country moving to alert Level 4 (after Delta community transmission was detected) from 20 August 2021.
While CV TAG advice was provided in the form of CV TAG memos, it is not possible for CV TAG to make comment on how and why its advice is used. By extension, it is also not possible for Manatū Hauora to make comment on why the government did or did not implement recommendations from its experts or advisors.”
Whilst this statement may be a valid explanation for a number of Covid issues which required a multi-agency response (for instance, in relation to MIQ), it seems inappropriate for Cabinet to stray from the technical advice of its vaccine advisory group on a fundamental clinical matter such as the interval between doses. Particularly when that advice is being given in order to reduce the risk of a serious (albeit rare) side effect.
Indeed, from first hand accounts, I am aware of some frustration from experts sitting on at least three technical advisory groups that their recommendations were not being implemented as part of the government’s Covid response. The Immunisation Implementation Advisory Group (IIAG) was so dissatisfied with the situation that it wrote to Dr Bloomfield in May 2021 to seek assurances from him that the group was still influential and that its recommendations would be “moving into Cabinet papers”.
One senior expert who sits on one of the advisory groups suggested to me that the government should have been transparent about the instances when it varied from the technical advice of its experts.
I note that CV TAG provided its memo to Dr Bloomfield on 21 July recommending that the dosing interval be extended to eight weeks. In a Written Parliamentary Question from National’s Chris Bishop, Minister Hipkins confirmed that the Ministry of Health (i.e. Dr Bloomfield and his steering group) provided advice to the Vaccine Ministers on 6 August recommending a six week interval which was agreed to by Cabinet on 12 August.
3. Who (individual or entity) made the request to CV TAG on or around 17 August to remove reference to dose intervals potentially providing some protection against myocarditis in public communications? From a public health perspective, why does the government consider that this was appropriate?
“On that date, evidence on the impact of intervals between doses on rare side effects was still emerging, and there was insufficient evidence to draw firm conclusions.”
This is an unconvincing answer from the Ministry. On 6 July, the minutes of the CV TAG meeting notes that the group discussed “the possibility of alterative vaccination schedules that might mitigate the risk in younger age groups”.
On 21 July, Medsafe issued an alert which stated, “It has now been concluded by Medsafe, other national regulators (such as the FDA) and the company, Pfizer, that myocarditis (inflammation of the heart muscle) is a rare side effect of vaccination with Comirnaty.” It also instructed Pfizer to update its data sheet for the safety signal.
On the same day, CV TAG issued its memo to Dr Bloomfield recommending extending the dosing interval to mitigate the myocarditis risk. CV TAG’s position on this issue has remained unchanged since July 2021. At the end of 2021 and beginning of 2022, CV TAG approved the 5 to 11 year old age group for vaccination and again recommended an eight week schedule specifically to reduce the myocarditis risk.
4. Did the government consult with CV TAG (or any other technical advisory committee) before it reduced the dose interval from 6 weeks to 3 weeks on or around 6 October and if so, what advice did it receive?
“In a meeting on 5 October 2021, CV TAG agreed that the default booking rules should be reduced to a three-week interval, due to the changing context of the Delta outbreak, the increased potential for circulating virus, and the urgent need for primary vaccine courses to be completed.”
There seems to be a discrepancy in the timing of advice. The Ministry has advised that the technical committee provided advice on 5 October, but in a Written Parliamentary Question from Chris Bishop on this specific point, Minister Hipkins responded that the Ministry of Health provided advice to Ministers about reducing the standard gap between doses on 4 October 2021. At this stage, it’s unclear if there is an error with the dates or if this was in fact another political decision that received a retroactive blessing from CV TAG.
It also appears to be an unusual recommendation from CV TAG because less than two weeks prior, the minutes from their 21 September meeting noted, “However, greater emphasis is needed on the benefits provided by longer dosing intervals, with CV TAG expressing concern that intervals of 3 weeks were becoming more common in Auckland’s outbreak.”
Chris Bishop questioned Minister Hipkins about this point, specifically asking “what was the concern from CV TAG around intervals of 3 weeks becoming more common in Auckland’s outbreak?” Hipkins’s response is below in which he references “higher antibody titres” but fails to mention the reduction in myocarditis risk which is the primary driver for CV TAG’s recommendation to retain the longer interval.
“I am advised that data had emerged that longer intervals between doses of the Pfizer vaccine produced higher antibody titres.
In August 2021, the standard gap between first and second doses of the Pfizer vaccine was extended from 3 to 6 weeks to ensure that partial protection was given to a larger number of people faster. However, a shorter time between the doses was still recommended in some cases, such as when people are at higher risk of contracting COVID-19, or for those who have a specific clinical treatment plan.
Since August, the Delta outbreak has increased the risk of contracting COVID-19 for everyone in New Zealand. Because of this increased risk, we are now advising every eligible individual in New Zealand to consider a shorter gap of 3 weeks between doses. Reducing this gap means more people can be fully vaccinated sooner, increasing New Zealand's community immunity.”
5. Given that the government followed the advice of CV TAG in relation to dose intervals for 5 to 11 year olds, setting it at eight weeks, on the basis of what formal advice did the government consider it appropriate for the dose interval between the first and second doses for 12 to 29 year olds to be set at 3 weeks?
“As detailed above, the advice for those agreed 12 years and older was based on CV TAG recommendations, which changed due to the changing context of the Delta outbreak, the increased potential for circulating virus, and the urgent need for primary vaccine courses to be completed.”
6. Did the government consult with CV TAG (or any other technical advisory committee) regarding appropriate dose intervals before it issued Vaccine Orders that in some cases required the dose interval between the first and second dose to be not more than 35 days (and in any event less than the 8 week interval recommended in CV TAG’s 21 July memo)? If yes, then what was that advice?
“Medsafe has approved a second dose of the Pfizer vaccine to be administered at least 21 days after the first dose, as seen in the Consumer Medicine Information Summary.
In the CV TAG memo dated 21 July 2021, it states: “People aged 30 years and over should still receive two doses of the vaccine at least 21 days apart.”
Furthermore, CV TAG also met on 27 July 2021 where dosing interval was discussed alongside the myocarditis recommendations updated. CV TAG discussed the recommended dosing interval for people under 30 years. CV TAG advised that while an 8 week interval is recommended for this age group, administering the second doses between 6 and 12 weeks is also acceptable, and that the exact timing is a programming decision.
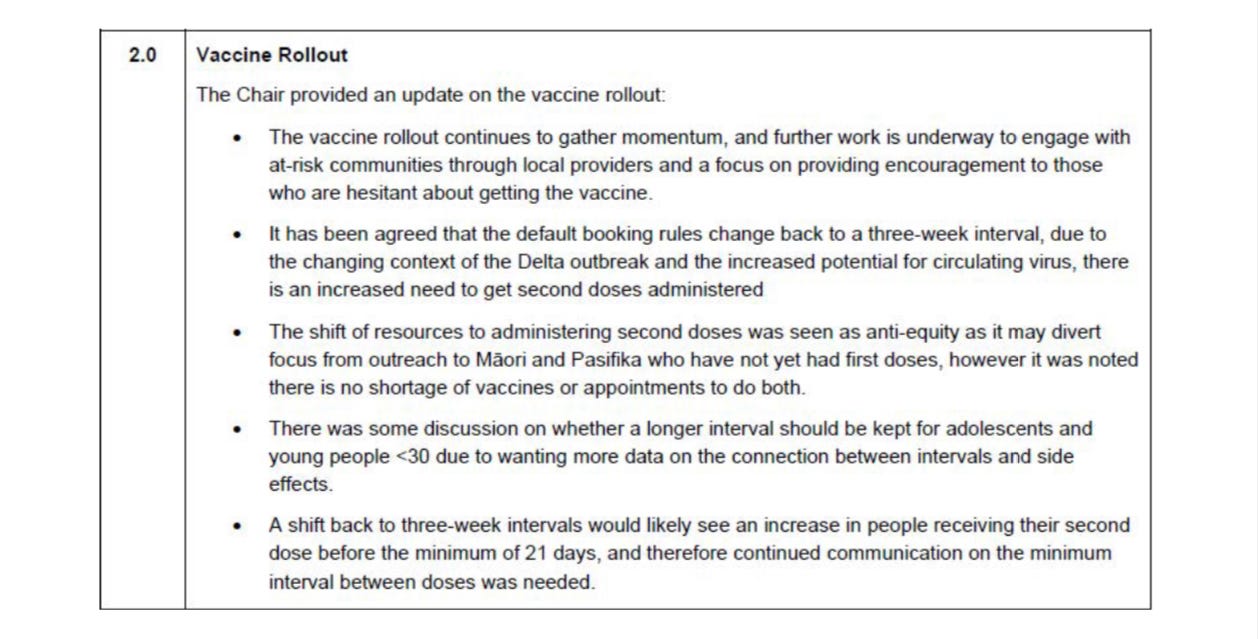
As stated above, in a meeting on 5 October 2021, CV TAG agreed that the default booking rules should be reduced to a three week interval due to the changing context of the Delta outbreak, the increased potential for circulating virus, and the urgent need for primary vaccine courses to be completed. An excerpt from the minutes of the meeting have been released to you and is set out below.”
Click image to view
It seems from this response that the government did not seek specific advice in relation to dosing intervals for the purpose of the mandates, some of which required no more than a 35 day gap between the two primary doses. That is obviously less than the 6 to 12 weeks recommended by CV TAG for people under 30.
The other point to note here is that when the decision to reduce the dosing interval was announced by Dr McElnay at the government press conference on 6 October she stated, “… and the technical advisory group has come back and said ‘yes, there never was any um, ah, safety concerns with um vaccinating at the three week’ and so from a practical, pragmatic perspective at this moment in time if you’ve had your first dose, and the only thing that’s stopping you from getting your second dose is waiting for a six weeks mark, the advice is that that can be done sooner ...”.
However, the minutes from the CV TAG meeting the day before (set out above) clearly states that there was an unresolved safety concern. The minutes note, “There was some discussion on whether a longer interval should be kept for adolescents and young people <30 due to wanting more data on the connection between intervals and side effects.”
Accelerating the pace of the vaccination rollout seems to have taken priority over other considerations. Indeed the minutes from an IIAG meeting on 5 August noted, “The critical nine-week peak period for COVID-19 vaccination will occur in September-October 2021. We need to maximise New Zealand’s demand during this period.”
CV TAG also anticipated that by reducing the interval back to three weeks some people will actually receive their second dose before the minimum 21 day period stipulated by Pfizer and approved by Medsafe. In response to a Written Parliamentary Question, Minister Hipkins confirmed:
“I am advised that 4,355 second doses have been recorded as given between 1 and 20 days after the first dose. This is less than 0.13% of second doses administered. Advice is provided to district health boards (DHBs) on next steps when a second dose is administered early. DHBs review early doses and put steps in place to mitigate the administration of second doses before 21 days have elapsed.”
7. In each of the High Court cases which considered the enforcement of mandates did the government fully disclose to the Court each instance where those mandates were not consistent with the advice of CV TAG?
“Expert evidence concerning the vaccine mandates was presented during each of the High Courts decisions, including evidence from Dr Ian Town and former Director-General of Health Dr Ashley Bloomfield. Any information that the Court deemed pertinent to its decision-making would have been presented to it, including details of CV TAG advice.”
I will publish any response from the Office of the Minister of Health if and when I receive it.
Thomas Cranmer, Lawyer with over 25 years experience in some of the world's biggest law firms. Thomas regularly blogs at https://cranmer.substack.com/
No comments:
Post a Comment
Thank you for joining the discussion. Breaking Views welcomes respectful contributions that enrich the debate. Please ensure your comments are not defamatory, derogatory or disruptive. We appreciate your cooperation.